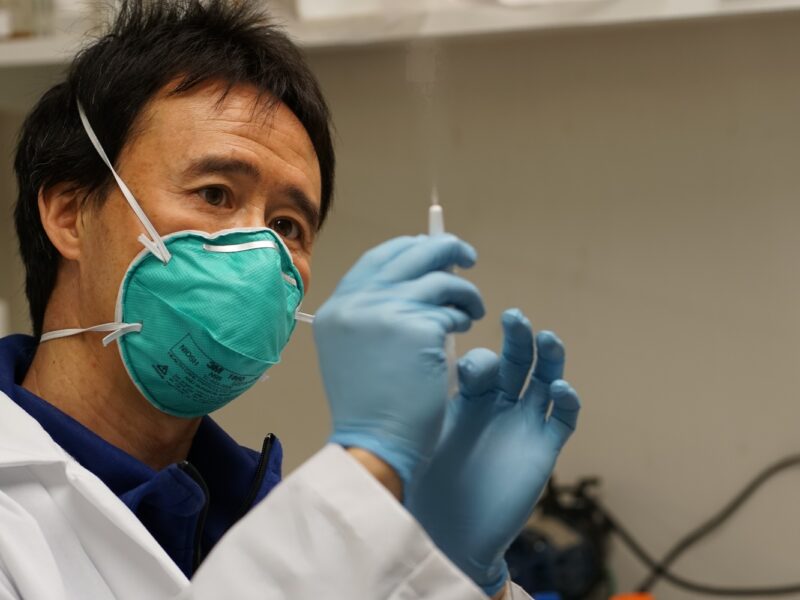
RaDVaC co-founder Don Wang
Greater Boston’s murky world of open-source COVID-19 vaccine research
Preston Estep is swirling a small vial of clear fluid in the back of a squat building outside Boston.
In early March, an all-consuming economic, political, and public health crisis upended the biomedical sciences. Eight months later, as the rest of us await the first doses of Pfizer’s promising mRNA vaccine, Estep may have already inoculated himself against the novel coronavirus nine or more times—at least, if he’s right about the contents of that vial.
The 59-year-old biologist is the founder of the Rapid Vaccine Deployment Collaborative, a group of scientists who have developed and self-administered a potential vaccine for SARS-CoV-2, the virus that causes COVID-19. Many of its members, including Estep, work under renowned geneticist George Church at the Harvard Personal Genome Project. In early July, the collaborative drew significant media attention when they shared a white paper describing a five-ingredient vaccine that they claim anyone with basic scientific training can make and take at home.
At least 40 people have taken the vaccine so far, with Church himself among the first.
It’s a gray Friday morning, and I’m at the lab where, seven months ago, Estep sprayed the original formulation of the vaccine into his nose. Cluttered with old computers and obscure equipment, the lab emits a low, soothing hum; it’s been home to Estep’s personal scientific projects since 2011, when he bought the space with RaDVaC co-founder Don Wang. Harvard’s Institutional Review Board doesn’t want self-experimentation in university labs, so this location has become RaDVaC’s headquarters.
I ask Estep how many doses are in the vial he’s holding, which contains the ninth and latest generation of the vaccine. He pauses for 30 seconds, calculating. Estep is tall, with a wiry way of moving, and the two inches of fluid look like nothing as he turns the vial in his long, gloved fingers. “Probably 400,” he says.
Over the past few months, RaDVaC has drawn harsh criticism from bioethicists for self-experimenting, lacking an independent ethics review board, and operating without large-scale, randomized clinical trials, the FDA’s gold standard for vaccine approval. These loose practices, some say, could do more than endanger a few researchers; they could undermine public trust in traditional SARS-CoV-2 vaccines in development by companies such as AstraZeneca, Pfizer, and Moderna. At the time of writing, there are four US vaccines in phase three trials, so why take unnecessary risks?
This criticism makes a lot of sense. But, at least on an emotional level, the simplicity of this image is unshakeable: A scientist holding 400 doses of potentially life-saving vaccine in his hand, as worldwide more than a million people have died from COVID-19 and in the US a third wave of infections rises. Add to the picture America’s failing healthcare system, the slow and unequal system of drug distribution, and pharmaceutical companies’ history of price gouging, and you start to wonder, What’s wrong with trying something different?
A lot and nothing at all. Like many moral questions, this one yields multiple answers—all of them high stakes, and most of them conflicting. Before wading too deep into the ethics, Estep helps me understand the science.
![]()
In developing their vaccine candidate, Estep says, his team followed “a complex algorithm balancing safety, effectiveness, simplicity of design, and simplicity of production.” The result of this algorithm was a nasal peptide vaccine.
It’s a design not unlike the flu mist—the major difference being that the flu mist includes whole weakened viruses, while RaDVaC’s product contains only virus subunits, called peptides. These peptides are protein fragments from the novel coronavirus, chosen for their predicted ability to stimulate long-lasting T-cell immunity. Because the vaccine doesn’t go directly into the bloodstream, it primarily creates mucosal, not systemic, immunity. But since the virus tends to invade the body through the nose and mouth, this nonbloodborne immunity may be enough to prevent it from entering the bloodstream.
A nasal peptide vaccine was the obvious match for Estep’s criteria. Safety: “Your nose is already not a sterile environment,” he says, so there’s a “much higher error tolerance.” Effectiveness: “There have been many human clinical trials using this basic design.” Simplicity of design: “There’s only five ingredients in the vaccine,” says Ranjan Ahuja, a co-founder of the collaborative and the director of community at the Personal Genome Project. Simplicity of production: “If this were a DNA or RNA vaccine,” Ahuja says, “that’d take more expensive equipment to produce.” To prepare the nasal peptide vaccine, nearly all you have to do is stir.
These last two claims—that the vaccine uses only five ingredients, and that you can make it at home—were what drew me, a layperson, to the project. The reality is a bit more complicated. Of the five ingredients—synthetic peptides, sodium triphosphate, water, salt, and chitosan—one is unlike the others: The peptide cocktail consists of nine individual peptides, each of which must be ordered from online vendors. Because of the fixed costs associated with peptide synthesis, these vendors only sell peptides in much larger quantities than the vaccine requires. The smallest quantity you can purchase makes thousands of doses and costs more than a thousand dollars—hardly practical numbers for lone-wolf enthusiasts.
Still, when Estep shows me how to prepare the vaccine, he makes it look easy. Hunched over a dead air workstation, he beckons me closer, and the sting of the 70% ethanol he used to sterilize his equipment filters through my mask.
“It’s extremely simple,” he says. “Really the most complicated part is adjusting the pH.” Early generations of the vaccine were too acidic (“like wasabi,” Ahuja recalls). Now, the collaborative adds sodium bicarbonate to raise the nasal spray’s pH to a near-neutral 5.5, which Estep says feels “just like water.”
Estep moves a long pipette rhythmically back and forth, combining the peptides into what he calls a “master mix.” Most of this mix will be frozen, along with the blood and mucus samples with which RaDVaC tracks its participants’ immune responses. Next, Estep activates his magnetic stir plate. On the plate is a beaker containing a solution of salt, water, and chitosan. A small tornado reaches down from the solution’s surface as the stir plate revs up to 500 rpm, whirring like a ceiling fan.
Chitosan—a carbohydrate derived from shrimp shells—is one of the vaccine’s key ingredients. From across the room, Ahuja explains that it’s an adjuvant; this means that chitosan helps trigger an immune response by mixing with the peptides to form tiny, jelly-like globules “at the same scale as a viral particle.” As Estep adds the peptide mix and sodium triphosphate, trillions of these nanoparticles clump invisibly together in the beaker. Ahuja compares them to droplets of oil in a vinaigrette.
After about 10 minutes of work, the vaccine is ready. Estep moves to the corner of the lab, where he first loads his finger-length sprayer with alcohol, spritzing it a few times to sterilize the nozzle. Then he adds the vaccine—one dose is about 500 microliters, according to the white paper. Stepping back, Estep removes his N95 mask, blows his nose, and raises the sprayer to his nostril. This dose will be followed by two boosters, spaced a few weeks apart.
When Estep administers the vaccine, squeezing the sprayer and inhaling sharply, he startles. “Oh, shit!” He’s forgotten to balance the pH, and the vaccine is more acidic than he expected. Despite the shock, Estep is buoyant, pointing toward Ahuja as if he’s won a prize: This mistake gives Estep his first opportunity to compare the pH-balanced and non-pH-balanced vaccines back to back.
“One of the interesting things about the history of science is how many little mistakes lead to great discoveries,” he says, laughing.
![]()
The history of science comes up often in conversations with the RaDVaC team. On our first Zoom call, after I told him that I study the discipline in college, Estep said, “Well, this is interesting history of science in the making, huh?”
But RaDVaC doesn’t overestimate its historical uniqueness. More than anything, the collaborative raises the past in order to claim continuity with scientific tradition. If you’ve read other articles about RaDVaC, this emphasis may come as a surprise. Commentators tend to identify RaDVaC with biohackers—an online community of DIY biologists, many of whom have an anti-regulatory ethos and lack conventional scientific training.
 Biohackers have had some success creating DIY alternatives to expensive medications, such as the Four Thieves Vinegar Collective’s $30 EpiPencil. But the biohacking community has also been the source of ill-fated attempts at SARS-CoV-2 vaccines. In June, biohacker Josiah Zayner recreated and self-tested a DNA plasmid vaccine that had shown promising results in animal trials, livestreaming the experiment on YouTube; by October, he had concluded that the messiness of human biology makes solo vaccine research impractical.
Biohackers have had some success creating DIY alternatives to expensive medications, such as the Four Thieves Vinegar Collective’s $30 EpiPencil. But the biohacking community has also been the source of ill-fated attempts at SARS-CoV-2 vaccines. In June, biohacker Josiah Zayner recreated and self-tested a DNA plasmid vaccine that had shown promising results in animal trials, livestreaming the experiment on YouTube; by October, he had concluded that the messiness of human biology makes solo vaccine research impractical.
In a March 9 email pitching the vaccine project to his future collaborators, Estep wrote that the pandemic might offer biohacking-style research its “best opportunity to date to make a very positive impact.” Eight months later, his collective draws a sharp distinction between the DIY methods of biohackers and RaDVaC’s open-source model. “This is modeled after free and open-source software projects,” Estep tells me, linking RaDVaC to established methods in computer science.
Speaking on a Make: magazine panel, Alex Hoekstra, another RaDVaC co-founder, said, “We want this work to be accessible to both biologists and engineers on every level, but the foundation of it is anything but amateur.” RaDVaC isn’t an opponent of pharmaceutical companies or the FDA; “Those people are our brothers and sisters,” Hoekstra insisted. The stated goal is sharing knowledge as quickly as possible—with individual citizen scientists, but also with businesses and universities, and even with the government.
What can be harder to stomach is RaDVaC’s self-experimentation, a process that involves Estep regularly drawing blood from his own leg to track his immune response. But this practice, too, has a surprising depth of precedent. “There’s a long history of self-experimentation,” Estep says, raising the example of Barry Marshall, who drank a live Helicobacter pylori culture to establish the cause of peptic ulcers, contracting a smelly, painful infection in the process. After performing a biopsy on himself, Marshall shared the 2005 Nobel Prize in Medicine for this research.
Susan Lederer, a University of Wisconsin-Madison professor of medical history and bioethics, gave me more examples of self-experimentation, both good and bad. “People who’ve been experimenting on themselves—who turn out to be right, and who turn out to be very wrong—are well-known in medical history,” she says.
If self-experimentation was once accepted, I ask Lederer, why has it become taboo? “There’s the idea that it clouds your vision, your objectivity,” she says, and “the idea that it fails to conform to our expectation of very well-defined inclusion and exclusion criteria” for test subjects in scientific studies. But she also mentions a darker notion: the idea that researchers’ lives matter more than those of regular people. Lederer tells me about Dr. Chester Southam, who injected elderly patients with live cancer cells in 1963. Asked why he didn’t experiment on himself, Southam said, “There are relatively few skilled cancer researchers and it seemed stupid to take even the little risk.”
Unsurprisingly, this attitude didn’t endear cancer research to the non-PhD-holding masses. That’s why Lederer argues, in some cases, self-experimentation can increase public trust in science. “I think for some individuals,” she says, “the willingness of researchers to go first, to inoculate their own children, means that they have a lot of confidence in their work”—a striking statement, because it’s almost the exact opposite of the charges of aggravating vaccine skepticism some bioethicists have leveled against RaDVaC.
Estep has made similar points to me on several occasions. He’s also argued that self-experimenting allows RaDVaC to update its design in light of new information about the virus, swapping out peptides here and there. If a paper came out that made AstraZeneca scientists want to modify their vaccine, they would need to restart the approval process, and their product might not return to human testing for months.
Yet when I bring up RaDVaC’s specific procedure, Lederer grows skeptical. “I’m not opposed to democratic science, and I think there is a place for citizen science,” she says, a question rising in her voice. “But I’m not sure I would want to be one of the first recipients of such a vaccine myself.”
![]()
Lederer is far from alone in her skepticism. Indeed, the Personal Genome Project’s own resident bioethicist, Jeantine Lunshof, has called RaDVaC an “ego trip.” When I tell my friends about the project, most react with a baffled curiosity that turns into concern the longer I explain.
One of the world’s top peer-reviewed journals, Science magazine, has featured two articles excoriating the collaborative. The first, published in August, casts RaDVaC as a media stunt, more likely to “sow mistrust of science” than produce well-evidenced results. The second, published in September, focuses on the ethical and legal regulation of DIY vaccine projects, arguing that institutional review boards and the FDA can and should intervene.
It’s hard to square these criticisms with the science-class atmosphere in the RaDVaC lab. Estep seems frustrated when I bring them up, turning from his workstation to look me in the eye.
The defense Estep offers is utilitarian: With real people dying every day, he argues that RaDVaC’s ability to update its design rapidly and share its findings widely outweighs the risks associated with its research methods.
“Thousands of people are on one track, and the train has already mowed down thousands, and we’re still trying to decide when to pull the lever and switch to the track with one person standing,” he says, referencing Judith Jarvis Thompson’s trolley problem thought experiment. “It’s insane.”
Estep insists he isn’t anti-big pharma, anti-vaccine testing, or anti-FDA—he just sees suffering and wants to make potential discoveries public, fast. He doesn’t seem to think science should operate like RaDVaC all the time, only when the benefits outweigh the costs. According to Estep, he and George Church plan to submit an article to Science magazine that responds to his critics with a version of this argument.
But Patricia Zettler doesn’t buy it. An associate professor at the Ohio State University Moritz College of Law, Zettler is one of the four authors of the September Science magazine article, titled “Self-experimentation, ethics, and regulation of vaccines.” She calls me from her department offices, which are mostly empty due to the pandemic.
“That’s a really tempting idea,” Zettler says, after I explain Estep’s thinking, “but I think it’s actually deeply misguided in many ways. A lot of the quote-unquote red tape we have—whether we have a regulatory body or not—is because science takes a long time, and it takes time to understand whether something really works or doesn’t.” In the long run, she thinks results obtained too quickly could become a source of confusion for scientists working toward “beneficial innovation.”
Zettler agrees that today’s vaccine research has a special urgency—but she draws the opposite conclusion from this fact. “To be clear,” she says, “our argument is not necessarily that do-it-yourself, non-establishment research efforts should be prohibited.” Rather, she thinks that in a time of crisis, it’s more important than ever for scientists to apply rigor in their research, lest anxious observers put too much faith in their results.
“Is it really self-experimentation,” Zettler asks, “when you’re engaged in activity that can have really pretty wide-reaching public health consequences … or might sow mistrust in other vaccine development efforts?”
![]()
In principle, Zettler makes a solid point. But as soon as I leave the RaDVaC lab, both sides of the question deflate a little in my mind. It’s started to drizzle, and most people are indoors; the few I pass on the street are wearing masks and jackets, hunched against the weather as if it’s any other day. The Massachusetts new case count has ticked up again, this time to 702.
RaDVaC hasn’t cured the novel coronavirus, and with vaccines from Pfizer and Moderna performing well in their final-phase trials, it’s unlikely it’ll make a major impact. But neither has the project jeopardized public health efforts, unleashed widespread distrust of vaccines, or impeded the work of other researchers—at least not in practice. Media coverage of RaDVaC has made a splash in certain circles, but when I mention it to people, they’re curious about the effort because none of them have heard of it.
Estep is more realistic about the practical position of his project than some might expect. Though many of RaDVaC’s test subjects have shown an uptick in mucosal immune markers, Estep knows his data isn’t yet statistically reliable. He would welcome corporate help in scaling up trials, but he says the biotech firms who have approached him “wanted to have approval over the release of RaDVaC information”—a constraint incompatible with his open-source ideals. Until better evidence arrives, the collaborative is clear that no one should change their behavior after taking their vaccine. “I still go out with two masks every day,” Ahuja tells me through both an N95 and a surgical mask.
But the neat conclusion that nothing matters leaves a huge question open. If RaDVaC neither proposes its methods as a radical revision to scientific tradition, nor expects its product to succeed through conventional channels, why do they continue to invite anger from bioethicists?
The answer may come from a brute fact on which Estep and his critics are forced to agree: the ongoing, unscientific horror of the pandemic. Estep becomes most animated when he remembers reading the news in early March—well before most Americans supported a lockdown—and imagining elderly Italian and Chinese people “quarantined completely alone, in a room to die, without any contact from their loved ones.” Thinking back to the 2003 Sars outbreak, Estep realized something it took most of us months to accept. “I knew this was very, very different.”
Whether or not it’s his main motivation, Estep seems to have caught onto something else before most: A commercial vaccine won’t protect many who need it most, at least not any time soon. He hopes that RaDVaC’s network of citizen scientists will be able to smooth the inequalities of the vaccine rollout in some small way, be it through the open-source availability of their research or a larger distribution apparatus built on that model. “Say you’re a small government in a central African country, and you know vaccines won’t be coming your way,” Estep says. “It’s really easy to make this—inexpensive too, to make and distribute it.”
After all, Pfizer’s much-heralded vaccine is far from inexpensive to make and distribute. It contains mRNA, a type of delicate genetic material that begins to break down outside of $10,000 ultra-cold freezers. Even if underfunded health systems, rural areas, and developing nations manage to obtain this equipment, Pfizer only expects to inoculate 15 to 20 million people by the end of the year. Competitor vaccines might increase the supply, but rich nations have already bought up 51% of doses of all leading vaccines, much as they did during the 2009 H1N1 pandemic.
The logic of the vaccine market is bleak—as long as scarcity persists, vulnerability to COVID-19 will fall unevenly across the familiar lines of geography, race, and class. Ahuja puts the situation more diplomatically, imagining RaDVaC as a supplement to a mainstream vaccine: “The dominating model of vaccine development has its strengths; ours, of course, has many as well.”
![]()
“This is a political problem!” says Pankaj Mehta, a physics professor at Boston University, so frustrated he’s almost yelling into the phone.
Mehta understands the emotional impulse behind RaDVaC—he’s no fan of big pharma, and he too watched thousands die in nursing homes, “murdered by neglect.” The urge to work outside the system is familiar to him. “I agree with open science,” Mehta says, but emphasizes that he’s “very skeptical that a small group of independent researchers can marshal the resources needed to safely develop and test a vaccine.”
The major limitation of RaDVaC, according to Mehta, is that we imagine it “as a technocratic solution to a political problem.” This is even true of conventional vaccines, he adds. I ask what he means. “I don’t think there’s going to be a vaccine that comes in and everyone has immunity, and then we’re back to our normal lives,” Mehta says. “I think this is another way of hiding the politics of the pandemic, which is basically balancing modern life on the backs of working-class people, asking them to do all the work and take all the risk.”
Mehta argues that our first duty is “to protect the elderly, the most vulnerable, to provide them healthcare and the means to survive.” Doing science differently does not necessarily lead to social progress, he insists; deploying a risky “untested vaccine” is no substitute for collective political action.
When I first started researching this story, I had a why-the-hell-not desire to take the RaDVaC vaccine. In the end, the collaborative didn’t offer me the opportunity to do so, but if they had, I’m not sure I would’ve gone through with it—not because I fear getting sick, or because I think RaDVaC is a historic monstrosity, but because taking the vaccine would give unearned closure to a story that remains deeply ambiguous.
As Mehta implies, there’s a wide gap between scientific knowledge and justice; it’s one health experts, political leaders, and activists must fill as they debate how to respond to the pandemic humanely. Even if RaDVaC is up to something valid, I’m not a frontline worker, a member of a group underrepresented in vaccine trials, or someone who could help upscale their testing. My participation would bring them no closer to moral clarity.
Last month, I spoke to one of those activists: Brian Cleary, a fellow at the Broad Institute of MIT and Harvard and an organizer with Free the Vaccine. He recently helped lead protests outside the Cambridge headquarters of Moderna, which has not yet committed to sharing its vaccine through the COVAX pool, despite receiving funding from the WHO-sponsored effort to distribute vaccines to developing nations.
“There’s some folks in Boston working on these issues,” Cleary says, “but it’s also kind of an international effort.” He goes on to discuss a few aligned groups—Universities Allied for Essential Medicines, the Center for Artistic Activism, and Science for the People. Another is the Open COVID Pledge, a Creative Commons-led effort to share vaccine-related intellectual property that RaDVaC endorses.
These groups share a number of concerns, from vaccine nationalism, to the exclusive licensing of pharmaceuticals, to the ways lockdown falls hardest on workers, people of color, and other marginalized communities. Cleary is perplexed by the indifference of some pharmaceutical companies to obvious inequality.
“They admit that this is the market failure,” he says, “and the crazy thing is that they’re so boxed into their thinking that they still think private enterprise and markets are the best thing.”
However unclear RaDVaC’s impact and ethics, it’s hard to find their basic way of thinking that objectionable. Cleary’s comment reminded me of a moment in their lab, when Preston Estep was mixing the vaccine, and Ranjan Ahuja sat off to the side, talking big ideas.
“To me, the essence of scientific progress is the creativity involved in stepping outside of the traditional bounds,” Ahuja said, grinning. It’s about asking, “How can we, again, improve this?”
Disclosure: The primary editor of this article, Nicole Aschoff, is the spouse of Pankaj Mehta.